|
 Stereotaxis
(from the Greek: 'spatial arrangement') is a surgical 'mentality'
rather than a surgical technique. The technique is based on using
the relationships between the 3D space occupied by brain lesions
and an external reference system to guide instruments to a pre-established
target. Stereotaxis
(from the Greek: 'spatial arrangement') is a surgical 'mentality'
rather than a surgical technique. The technique is based on using
the relationships between the 3D space occupied by brain lesions
and an external reference system to guide instruments to a pre-established
target.
In 1949 the Swedish neurosurgeon Lars Leksell devised a stereotactic
'helmet' for human functional neurosurgery. After the advent of
computerized imaging, the procedure was applied to various branches
of surgery (biopsies of deep thoracic and abdominal masses, of non-palpable
mammary nodules etc.). He later developed the concept of 'radiosurgery',
which aimed at destroying discrete anatomical regions within the
brain while sparing surrounding healthy tissues. However, it wasn't
until the end of the 1960s, with the introduction of the first linear
accelerators and their refinements in the 1980s, that Dr.  Leksell's
idea was put into practice, and research centers in Boston (US)
and Vicenza (Italy) developed the technique of stereotactic radiation
with accelerators. Leksell's
idea was put into practice, and research centers in Boston (US)
and Vicenza (Italy) developed the technique of stereotactic radiation
with accelerators.
Brain stereotactic radiotherapy was first applied to very small,
deep lesions, which were not surgically treatable, e.g. vascular
lesions. Subsequently, lesions as large as 3 cm or more in diameter,
which is often the case of brain tumors and metastases, were treated.
Used also for non-tumoral diseases (e.g. angiomas, aneurisms, malformations),
stereotactic radiotherapy has become the treatment of choice for
many cerebral neoplasias.
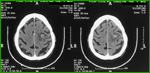 Pre-treatment
Pre-treatment
computerized tomography |

Post-treatment
computerized tomography |
Method
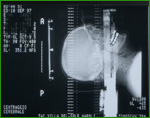
 Leksell's
stereotactic device consists of a helmet that is fixed to the patient's
head with pins. Radio-opaque or paramagnetic samples are inserted
into the helmet. Then, a three-dimensional space is defined with
computerized tomography and magnetic resonance, and the tumor's
coordinates are established on this 3D space. Thus, the stereotactic
helmet serves to locate the exact position of the tumor and, subsequently,
to administer the radiations exactly on the tumor area. Leksell's
stereotactic device consists of a helmet that is fixed to the patient's
head with pins. Radio-opaque or paramagnetic samples are inserted
into the helmet. Then, a three-dimensional space is defined with
computerized tomography and magnetic resonance, and the tumor's
coordinates are established on this 3D space. Thus, the stereotactic
helmet serves to locate the exact position of the tumor and, subsequently,
to administer the radiations exactly on the tumor area.
Fixation
device

Invasive |

Non-invasive |
Today,
we use a non-invasive device called the 'stereotactic relocatable
frame' instead of Leksell's helmet. This frame provides the stereotactic
location, degree of immobilization and precision necessary for radiosurgery.
It consists of a helmet that can be adapted to align precisely the
laser and the positioning of the isocentric site of the linear accelerator.
Using dental impression material, we make a cast of the patient's
mouth (mouthpiece). The mouthpiece is attached to two moveable arms
on the frame, and fits comfortably into the patient's mouth. In
addition, a thermoplastic cast is made of the patient's face and
head. When fitted with the thermoplastic mask and with the mouthpiece
comfortably in place, the patient is immobilized so as to ensure
the millimeter reproducibility of treatment.
Treatment
steps
 The
stereotactic helmet is fixed to the patient's head under local anesthesia.
The patient feels no pain. The
stereotactic helmet is fixed to the patient's head under local anesthesia.
The patient feels no pain.
 Then
examinations such as computerized tomography, magnetic resonance
and angiography are performed to locate, diagnose and measure the
neoplastic mass. Then
examinations such as computerized tomography, magnetic resonance
and angiography are performed to locate, diagnose and measure the
neoplastic mass.
 Subsequently,
the treatment strategy is planned at the computer. During therapy
the linear accelerator moves in synchrony with the treatment bed. Subsequently,
the treatment strategy is planned at the computer. During therapy
the linear accelerator moves in synchrony with the treatment bed.
 Using
the computerized volumetric reconstructions, we simulate various
surgical approaches. We also evaluate the best way to reach a target
in case of obstruction by nerve or vascular structures. Besides
simulating surgery, it is possible to plan and perform the surgery. Using
the computerized volumetric reconstructions, we simulate various
surgical approaches. We also evaluate the best way to reach a target
in case of obstruction by nerve or vascular structures. Besides
simulating surgery, it is possible to plan and perform the surgery.
Supine
on a bed, with the helmet well-centered, the patient is irradiated
for 15-20 minutes, with the radiation source that circles according
to a prefixed scheme, so that the rays reach the tumoral target
from various directions, following different pathways each time,
so as to spare healthy tissue as much as possible.
Conclusions
Radiosurgery is used to treat:
-
malformations, small benign neoplasias that are difficult to reach
and remove (auditory neurinomas, meningiomas of the base of the
skull, pinealomas);
- single and multiple encephalic metastases;
- such diseases as thalamotectomy for Parkinson's disease, refractory
pain etc.
The
mortality and morbidity of stereotactic procedures are very low,
in the order of 1% and 2%, respectively, whereas the mortality of
free-hand biopsy for malignant neoplasias reaches 13%.
Described simply, stereotactic radiotherapy may seem banal. But
it requires a high level of expertise, organization and an interdisciplinary
approach: radiotherapists, health physicists, neuroradiologists
and neurosurgeons closely interact during this procedure.
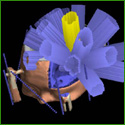
Dose released with
conformational beams |
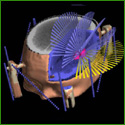
Dose released with
arc therapy |
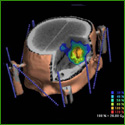
Result of the 3D
distribution |
A
single stereotactic radiotherapy session may be sufficient, or the
dose can be divided into various sessions. Stereotactic radiotherapy
can be used to treat deep-sited neoplastic masses, which cannot
be treated surgically because of the risk of damaging important
cerebral areas. In addition, the technique can be applied to slow-growing
tumors so as the do not reach a size that is difficult to treat
surgically. With the advent of stereotactic radiotherapy it has
become possible to cure the 'very small' and the 'very deep'.
Stereotactic radiotherapy can be applied also to larger brain tumors.
After the neurosurgeon has removed as much of the tumor as possible,
stereotactic radiotherapy can be used where surgery might cause
damage. Radiosurgery is now being applied to other types of tumors,
such as chest and abdomen tumors.
|